Definition
- Fracture of the distal fibula at the lateral aspect of the ankle joint.
- Is classified according to its relation to the syndesmosis between the distal tibia and fibular.
Aetiology
- Commonly associated with rotational injuries of the ankle, this can occur either as an inversion or eversion injury. Weber B ankle fracture most commonly associated with SER (supination, external rotation) injuries.
- Sports injuries or falls while walking most common cause for ankle fractures.
- Often associated with increased BMI and smoking.
Epidemiology
- Ankle fractures occur in roughly 187 people per 100,000.
- Unimalleolar ankle fractures (lateral and medial) account for 60-70% of all ankle fractures.
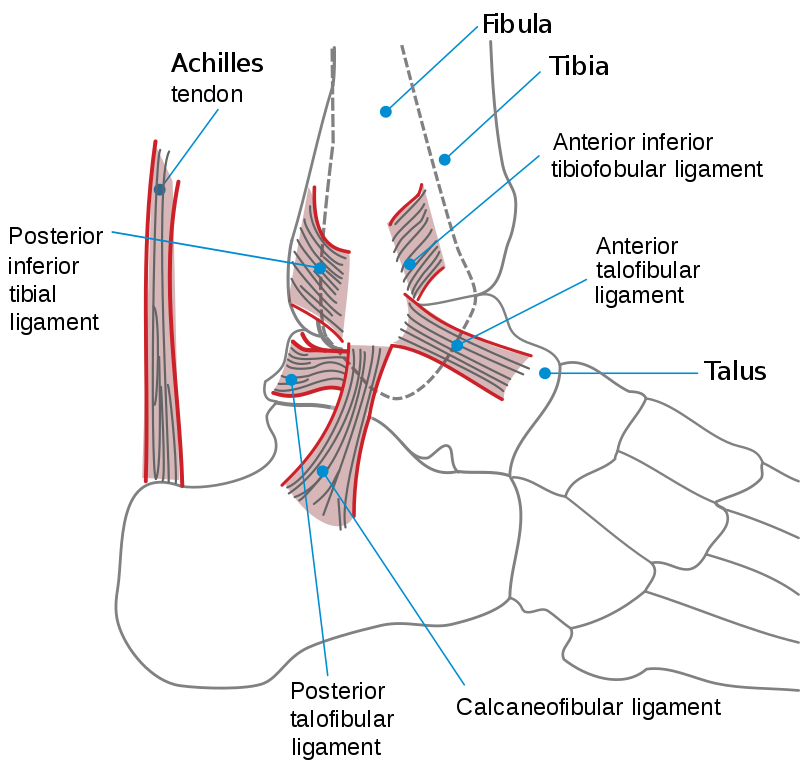
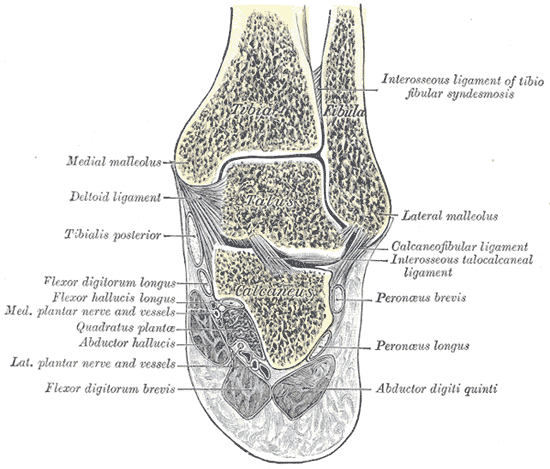
Anatomy
- The lateral malleolus is a core component of the talocrural joint, also known as the ankle joint.
- This joint is comprised of the tibia (providing the plafond and medial and posterior components), the fibula (providing the lateral component) and the talus.
- The distal tibia and fibula provide a rectangular socket (termed the mortise) that articulate with the talar trochlea.
- This joint acts as a mortise and tenon joint
- A membranous ligament spans between the tibia and fibular termed the interosseous membrane. The distal aspect forms the tibiofibular ligament forming a syndesmotic joint.
Pathology
- Most common fracture pattern is transyndesmotic (Weber B) accounting for over 50% of all isolated lateral malleolar ankle fractures.
- Infrasyndesomtic (Weber A) next common at ~25% and then Suprasyndesmotic (Weber C) accounting for approximately 15%.
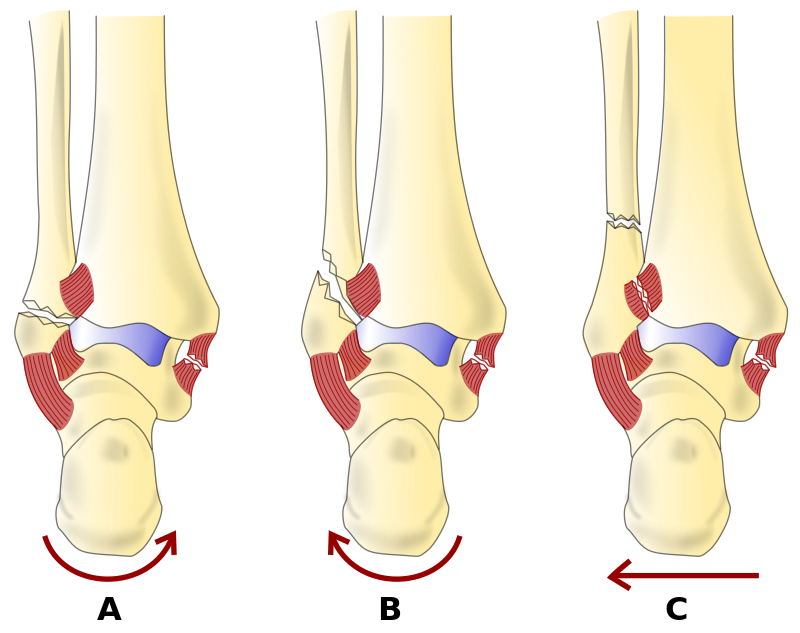
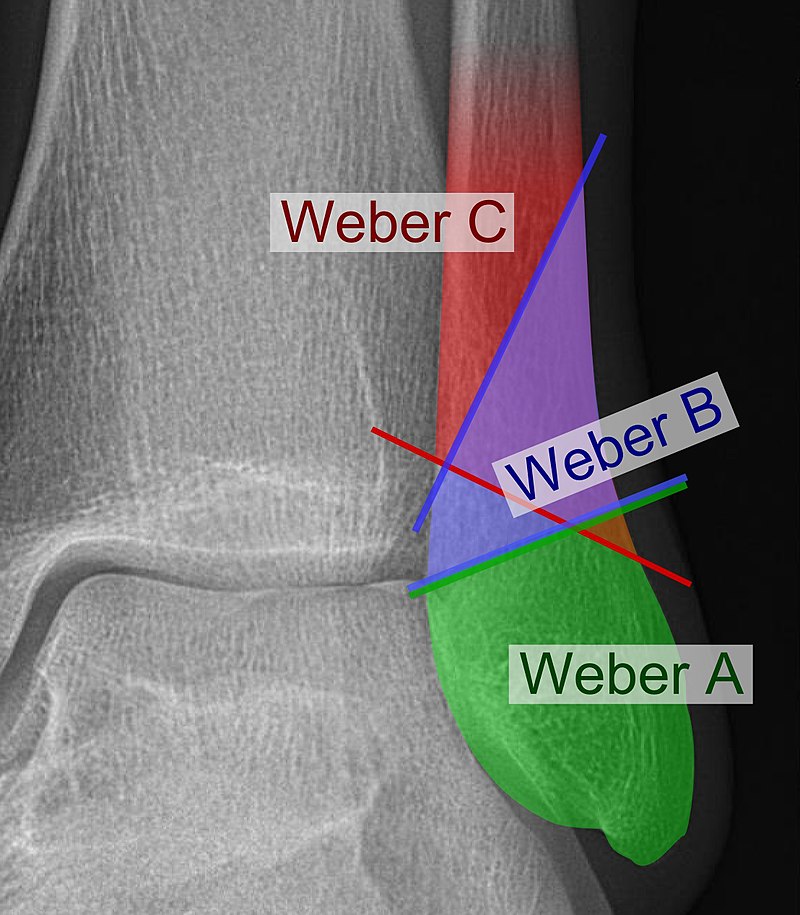
Classification
Danis Weber Classification
| Weber Classification | |
| Weber A | Infrasyndesomtic- Fracture occurring below the distal tibiofibular ligament. Indicates the talocrurual joint is likely stable. |
| Weber B | Transydesmotic- Fracture occurring through the level of the distal tibiofibular ligament. Indicates the talocrural joint has the potential to be unstable. |
| Weber C | Suprasyndesmotic -Fracture occurring above the level of distal tibiofibular ligament. Indicates that the talocrural joint is likely unstable |
The Danis Weber classification is a useful system to simply separate out isolated lateral malleolar fractures into understandable fracture patterns and thus management. The classification system also helps indicate prognosis post injury.
History
- Most common symptoms are pain in the ankle, primarily along the lateral side of the ankle and pain with movement/weight bearing on the affected side.
- Most commonly occurs after inversion/eversion injury of the ankle
- Patient may present reporting they assumed it was “just a strain or sprain but pain didnt improve”
Examination
Inspection
- Swelling of ankle
- Rare to have deformity,
Palpation
- Tenderness along the lateral aspect of the ankle
Movement
- Pain on movement of ankle
- Inability to properly weight bare
Investigations
XR
- First line investigation for lateral malleolus fractures.
- Requires AP, Lateral and Mortise views.
- Ensure ankle is within the joint. Any subluxation or dislocation requires early reduction.
- Appropriate views to determine potential associated medial malleolus/posterior malleolus.
- Important to determine not only the presence of a fracture but also review for tibiotalar instability (Syndesmosis instability) as any tibiotalar instability is a strong determinant for operative management.
- Consider imaging of full tibia and fibula as well for potential fracture proximally (eg Maisonneuve fracture) due to the strong interosseous membrane transmitting force across both bones.
(importance of XR views being standardized)
CT
- Not a routine imaging test for isolated ankle fractures however can be used to further clarify fracture patterns for operative management if unclear on original imaging.
- Useful to determine any other fractures not easily identified on original plain radiographs including fractures through the medial malleolus, posterior malleolus, tibial plafond or talus.
Differential Diagnosis
- Ligamentous injury
- ATFL/Calconeofibular/PTFL
- Bimalleolar fracture
- Trimalleolar fracture
- Foot fractures
- Talus/Calcaneus etc
Treatment
- One of the most important aspects of any ankle fracture is to determine if the talus is within the mortise. If there is incongruence with the joint then early closed reduction and plaster of the ankle joint is necessary. This not only aids with pain and swelling but also prevents any further damage to the congruent surfaces. This does not need to be definitive management but will provide time to organise appropriate management as required.
Non Operative
- Appropriate for Weber A and some Weber B fractures. The appropriateness of non operative management is determined primarily by the stability of the ankle joint and the displacement of the fracture.
- Patients who are also poor candidates for surgery or non ambulatory may also be considered for non operative management.
- This non operative treatment is very often achieved through casting but other methods including boot/splinting can also achieve this.
- Reduction and casting technique
Operative
- Appropriate for Weber C and most Weber B fractures. This is due to the inherent instability of these fractures.
- Patients who have higher functional demands, including younger or more active people should also be considered for surgery with fractures that could be managed either way due to the higher demands they will impose of the lateral malleoli.
- For isolated lateral malleolus plating is the most common method (link to operation) also being appropriate for patients with a small distal fragment.
Surgical Technique
(Approach- to be added)
Lag Screw and Neutralisation plate
Complications
- Uncommon in appropriately treated isolated lateral malleolar fractures.
- Increased risk of complications occur with diabetes/smoking, poor compliance with weight bearing restrictions or poor engagement with physiotherapy once movement allowed.
Prognosis
- Prognosis of this injury is heavily determined by the appropriate diagnosis and treatment
- Most important aspect for prognosis is by retaining acceptable ankle congruence. Failure to do so can lead to arthritis.
References
Aiyer, Amiethab A. MD; Zachwieja, Erik C. MD; Lawrie, Charles M. MD; Kaplan, Jonathan R. M. MD Management of Isolated Lateral Malleolus Fractures, Journal of the American Academy of Orthopaedic Surgeons: January 15, 2019 – Volume 27 – Issue 2 – p 50-59 doi: 10.5435/JAAOS-D-17-00417
Daly PJ, Fitzgerald RH Jr, Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand. 1987 Oct;58(5):539-44. doi: 10.3109/17453678709146395. PMID: 3425285.
Goost H, Wimmer MD, Barg A, Kabir K, Valderrabano V, Burger C. Fractures of the ankle joint: investigation and treatment options. Dtsch Arztebl Int. 2014;111(21):377-388. doi:10.3238/arztebl.2014.0377
Jensen SL, Andresen BK, Mencke S, Nielsen PT. Epidemiology of ankle fractures. A prospective population-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand. 1998 Feb;69(1):48-50. doi: 10.3109/17453679809002356. PMID: 9524518
Kennedy JG, Johnson SM, Collins AL, DalloVedova P, McManus WF, Hynes DM, Walsh MG, Stephens MM. An evaluation of the Weber classification of ankle fractures. Injury. 1998 Oct;29(8):577-80. doi: 10.1016/s0020-1383(98)00116-8. PMID: 10209586.
Kilian M, Csörgö P, Vajczikova S, Luha J, Zamborsky R. Antiglide versus lateral plate fixation for Danis-Weber type B malleolar fractures caused by supination-external rotation injury. J Clin Orthop Trauma. 2017;8(4):327-331. doi:10.1016/j.jcot.2017.06.005
Lindsjö U. Operative treatment of ankle fractures. Acta Orthop Scand Suppl. 1981;189:1-131. doi: 10.3109/ort.1981.52.suppl-189.01. PMID: 6787831.
Marsh, JL, Saltzman, CL. Ankle Fractures. In: Rockwood and Green’s Fractures in Adults, Bucholz, RW and Heckman, JD (Eds), Lippincott Williams and Wilkins, Philadelphia 2002. p.2001.
Author Contribution
Dylan Ellis, Orthopaedic Resident, 2021