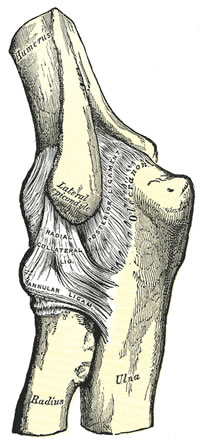
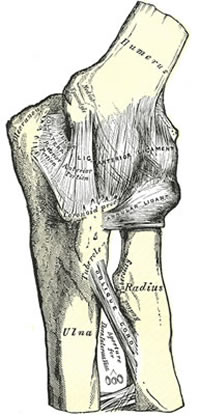
Valgus stress & palpate Medial Collateral Ligament
Investigations
Xray
before & after reduction
widening of joint space indicates osteochondral fragments
CT Scan
if unable to reduce or suspicious of fracture / intraarticular fragment
Treatment
Initial
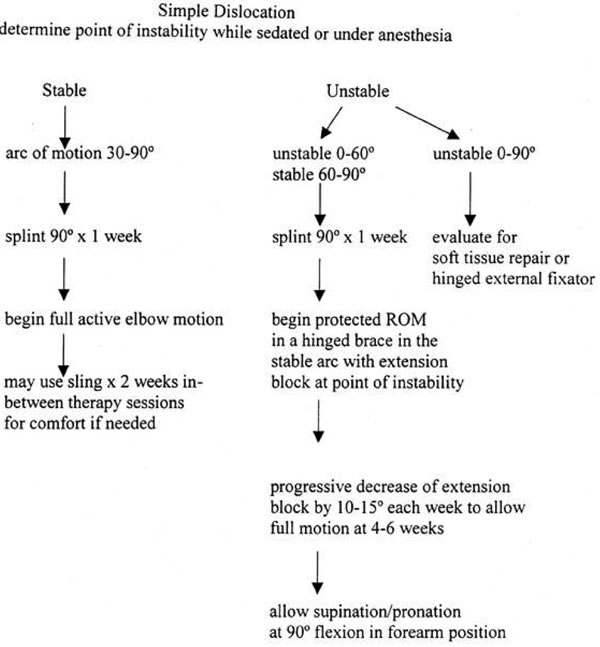
Post reduction assess stability + re-Xray + splint
Repeat Xray at week 1 to document reduction
If reduction is concentric & stable
gentle ROM exercises at 5-7 days, with sling for comfort
Aggressive therapy is associated with HO
Prolonged rigid immobilisation leads to poor ultimate range
ROM exercise within stable range initially
If mark instability
immobilize in sufficient flexion
Gradual extension from day 7
followed by gradual progression over next 3 to 4 weeks
Pronation also helps with stability
Flexion returns first, extension improvement can continue for upto 12 months
Recurrence 1 -2 %
Operative Treatment
Immediate closed reduction with GA
Longitudinal traction at 45° flex (to unlock coronoid) with direct pressure on Olecranon to assist
Estimate where stable & allow movement in that arc for 1/52
Then mobilize
If FFD at 6/52 > 40° then night extension splint
Will achieve :
80% at 3/12
100% at 12/12
Complete Dislocation with Radial fractures
Poor outcome if immobilized >4/52
Treat fractures according to type
Mason I = Reduce elbow
Mason II = ORIF
Mason III = Excise & Hinge splint
If Medial Collateral Ligament or Interosseous membrane (Essex-Lopesti fractures) injury, then need to insert spacer to avoid migration of Radial remmnant
Complete Dislocation with Coronoid fractures
See Morrey Class
Poor outcome related to fragment size ie Type II & III
>50% of coronoid
Leaves humero-ulnar articulation unstable
Complete Dislocation with Olecranon fractures
TBW or Neutralization Plate
Open reduction & Repair of Ligaments
Indications
All complete elbow dislocations result in medial + lateral ligament rupture but rarely is surgery indicated
Prospective studies show no advantage in early collateral ligament repair over early ROM
Indications for surgery
Flexion >50˚ required to maintain reduction
Associated unstable fracture
Operative procedure
Protect ulna nerve
Repair Medial Collateral Ligament + flexor/pronator mass, usually from humeral origin by intraosseous sutures or suture anchors
Radial head ORIF = preserve posterior fibres Lateral Collateral Ligament complex (Lateral Collateral Ligament blends with the annular ligament laterally to insert on the proximal ulna
Incision is made anterior to midline of radial head, to preserve posterior fibres of Lateral Collateral Ligament)
Coronoid fracture = ORIF when >50% coronoid process fracture (note brachialis inserts coronoid base)
Complications
Stiffness
Most patients lose terminal 10-15˚ extension
Early active ROM prevents anterior capsular scarring
Consider elbow capsular release after 6 months
Heterotopic Ossification
Ectopic ossification = mature bone formation in nonosseous tissues
75% of cases
HO that limits ROM <5%
Common sites = brachialis, collateral ligaments
Associated with aggressive ROM therapy, closed head injury
Resection is best delayed until ossification is matured on radiographs
DRUJ Instability
Essex-Lopresti lesion (originally described radial head fracture, dislocated DRUJ, without elbow dislocation)
Lateral Elbow Instability
Posterolateral rotatory instability occurs principally in supination
Xray = posterior radial head subluxation + ulnohumeral joint widening