scapular fracture combined with an upper humerus fracture or a clavicular injury
true floating shoulder does not occur unless, in addition to a clavicular shaft fracture:
scapular spine/acromial fracture
or disruption of the acromioclavicular (AC) & coracoacromial (CC) ligaments
Anatomy
coracoacromial (CA) ligament
is an important stabilizer of glenoid neck fractures because it is the only direct ligamentous connection between proximal & distal
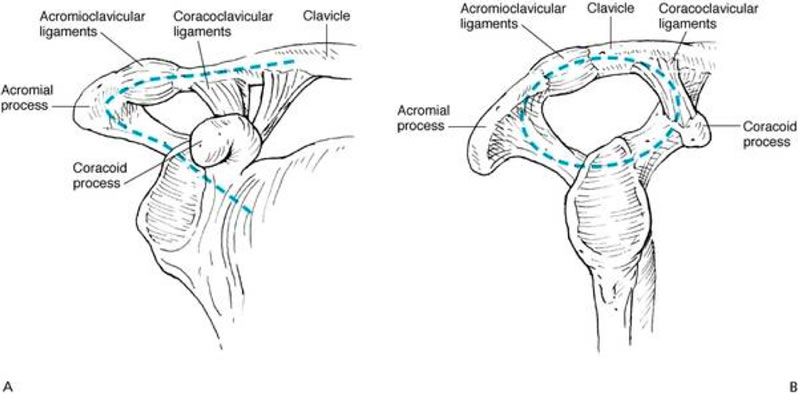
Superior Shoulder Suspensory Complex (SSSC)
bony/soft tissue ring composed of
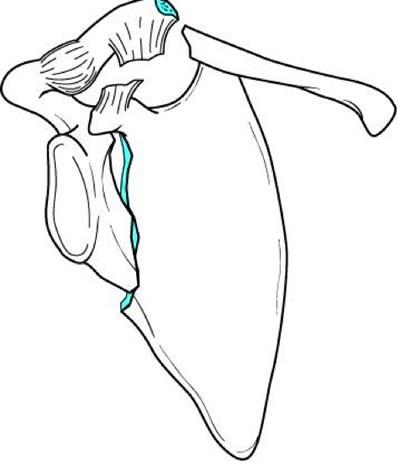
glenoid
coracoid
acromion
distal clavicle
connecting ligaments
Maintains the stable relationship between the upper extremity & the axial skeleton
Isolated, single traumatic disruptions are common (e.g., grade II acromioclavicular separation) & do not significantly change the stability of the ring
Double disruption is failure of the ring in two or more places & results in delayed healing, ↓ strength, & other long-term problems
Single soft tissue disruption + clavicle fracture or the body/spine of scapula
may produce the same result as double disruption
Glenoid neck fracture + either an AC separation or a clavicle fracture
double disruption of the SSSC, creating a need for surgical restoration of stability
Pathology
ipsilateral clavicular & scapular neck fractures:
weight of the arm & the muscle pull allow the glenoid to move anteromedially, leading to ptosis of the shoulder
Treatment
Such complex injury patterns could lead the clinician to consider stabilizing one or both fractures
For displaced fractures, operative intervention should be considered for
medial glenoid displacement of greater than 3.0 cm
clavicle displacement that meets indications for open reduction
multiple trauma with the need for upper extremity weight bearing as soon as possible
greater than 40° of abnormal glenoid version
Patients can do well with clavicular fixation alone