Written by Dr Josh Petterwood MBBS | Accredited Orthopaedic Registrar
Weekly Presentation – 5th March 2010
Introduction
- Infrequently performed procedures
- Little research
- Complex conditions
- Complex operations
Cerebral Palsy
- Issues
- Dysplasia/subluxation/osteoarthritis
- Bony abnormalities
- Coxa valga,
- persistence of foetal anteversion,
- superior subluxation
- Secondary to muscle imbalance
- Tight flexors/adductors overpower weak abductors/extensors
- Evidence
- 2 studies • 19pts • 16pts
- 2 case reports
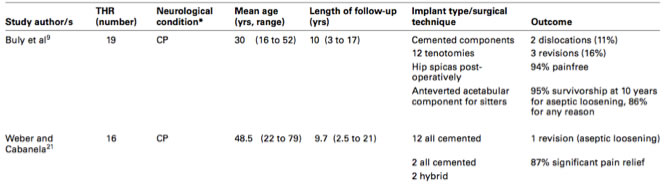
- Results
- Resection arthroplasty and arthrodesis mixed results
- Theoretically THR
- High risk of dislocation and aseptic loosening
- Management
- Custom implants,
- constrained implants,
- post op hip spicas,
- concurrent tenotomies/botulinum
- Multi-disciplinary approach
Parkinson’s
- Epidemiology
- Common disease – 1%
- Rigidity,
- contractures,
- bradykinesia,
- tremor,
- dystonia,
- postural instability
- Results
- Hemiarthroplasty performed frequently
- High mortality (up to 47% at 6/12)
- High morbidity secondary to medical comorbidities
- Little evidence regarding THR Parkinson’s
- Scottish National Arthroplasty Registry
- 2394 patients
- Significantly lower dislocation rate
- Weber et al
- 107 pts – 93% pain relief – 26% medical complication
- Did well early, then deteriorated
Poliomyelitis
- Issues
- Flaccid paralysis
- Dysplasia,
- subluxation,
- osteopaenia,
- contractures,
- leg length discrepancy
- Results
- THR infrequently performed
- Literature confined to case reports
CVA
- Results
- Scottish National Arthroplasty Registry
- Desreased risk of dislocation
- Increased risk of HO
- Scottish National Arthroplasty Registry
Spinal Injury
- Increased risk of HO
- Radiation/indomethacin recommended
- Increased dislocation risk in sitters eg. paraplegics
Charcot
- Case reports only
- Usually contraindicated Spinal Injury
Discussion
- Older pts with Parkinson’s/CVA
- Lower functional demand
- Less chance of dislocation
- Off-the-shelf, unconstrained implants
- High incidence of medical comorbidity
- Younger pts with CP/polio/spinal injury
- Higher incidence of dislocation
- High variability in anatomy
- Constrained, modular implants
Take home message
- Complex patients requiring
- Individualised approach
- Careful pre operative planning
- Consideration of deforming forces across joint
- Procedure
- Templating
- Modular prostheses
- Constrained acetabular components
- Soft tissue procedures/balancing
- Multi-disciplinary approach
- Pre and post op
- Good outcomes achievable
- Pain
- Function