General
- Synovial joint
- Modified hinge joint
- Movements
- Flexion
- Extension
- Rotation
- Compound joint
- 2 condylar joints between femur and tibia
- Sellar joint between patella and femur
Components
Capsule
- Attachments
- Anterior
- Deficient above the level of the patella
- Allows the suprapatellar bursa to be in communication with the joint
- TIbial tuberosity distally
- Posterior
- Proximal margin of femoral condyles and in the intercondylar area to the distal edge of the groove for the PCL
- Attachment to the lateral condyle is interrupted by an aperture for the popliteus tendon
- Medial
- Articular margin of femur
- Thickening is a deep component of the MCL firmly attached to the medial meniscus
- Lateral
- Proximal to the groove for the popliteus tendon
- Head of the fibula
- Anterior
Ligaments
Tibial collateral ligament (medial ligament)
- Flat triangular band
- Attachments
- Proximally to the medial femoral epicondyle, just distal to the adductor tubercle
- Distally to the upper part of the medial surface of the tibia
- Anterior margin is free except at attached extremities
- Posterior apex blends with capsule, attached with medial meniscus
- Above distal attachment
- Crossed by sartorius, gracilis and semitendinosus
- Deep to distal part
- Medial inferior genicular vessels and nerve
- Anterior expansion of semimembranosus tendon
Fibular collateral ligament (lateral ligament)
- Cord-like
- Attachments
- Proximally to lateral epicondyle, below the attachment of the lateral head of gastrocnemius and above the tendon of popliteus
- Distally to head of fibula overlapped by the tendon of the biceps femoris
- Not attached to the capsule
- Not connected to the lateral meniscus
- Tendon of popliteus lies deep to the capsule here
- Lateral inferior genicular vessels and nerve run deep
Oblique popliteal ligament
- Expansion from the tendon of semimembranosus
- Blends with the capsule at the back of the joint
- Ascends laterally to the intercondylar fossa and lateral femoral condyle
- Popliteal artery lies on it
- Genicular vessels and nerves penetrate it
Arcuate popliteal ligament
- Y shaped thickening of posterior capsular fibres
- Stem is attached to head of fibula
- Medial limb arches over tendon of popliteus to posterior edge of tibial intercondylar area
- Lateral limb ascends to lateral femoral condyle
Cruciate Ligaments
- Lie within the capsule, but not within synovial membrane
Anterior cruciate ligament (ACL)
- Twists on itself
- Attachments
- Distally to anterior part of the tibial plateau
- Between attachments of the anterior horns of the medial and lateral menisci
- Proximally to posteromedial aspect of lateral femoral condyle
- Distally to anterior part of the tibial plateau
- Can be divided into 2 functional and anatomic bundles based on tibial insertion sites
- Anteromedial bundle (AM) – tight in flexion
- Posterolateral bundle (PL) – tight in extension
- Blood supply via branches of middle geniculate artery
- Clinical significance is that if one bundle intact or other bundle partially torn, can consider treating conservatively
- ACL reconstruction
- Graft options
- Autograft
- Middle third BPTB
- 4 strand hamstrings
- Quadriceps tendon
- Allograft
- Synthetic
- Autograft
- Tunnel placement
- Tibial tunnel
- 7mm anterior to PCL and central
- Posterior 1/2 ACL footprint
- 2/3 of the way towards medial tibial spine from anterior horn of lateral meniscus
- 55 degree angle
- Femoral tunnel
- 2 o’clock (R knee) or 10 o’clock (L knee)
- Want to be posterior
- Want 2mm of back wall behind tunnel
- Tibial tunnel
- Graft options
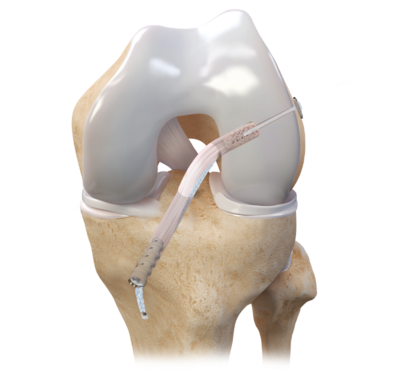
Image source: Arthrex
Posterior cruciate ligament (PCL)
- Shorter, stronger, broader
- Attachments
- Distally to smooth impression on posterior part of the tibial intercondylar area
- Proximally to the anterolateral aspect of the medial femoral condyle
Examination
- Anterior Drawer Test
- Knee in 90 degrees flexion
- In ACL injury, tibia translates forward and the endpoint feels soft
- More specific for injury of anterior fibres
- Lachman’s Test
- Knee in 20 to 30 degrees of flexion
- Examiner pulls forward on tibia while pushing backwards on the femur
- In ACL tear
- Translation is increased and endpoint indefinite
- In incomplete ACL injury
- Increased anterior laxity but firm endpoint
- More specific for injury for the posterior portion of the ACL
- Pivot Shift Test
- Examiner lifts the lower limb off the table by the foot and internally rotates it
- In non functional ACL
- Gravity causes femur to fall posteriorly
- Resulting in anterior subluxation of the tibia
- Examiner then applies a valgus stress to the proximal tibia, as well as flexing the knee
- Between 20 – 30 degrees, the tibia spontaneously reduces
Menisci
- Crescentic discs of fibrocartilage
- Triangular in cross section, thicker in their convex periphery
- Distal surfaces are flat, proximal surfaces are concave
- Mainly avascular but peripheral zone is vascularised by capillaries from the capsule
Medial meniscus
- Almost a semicircle, broader posteriorly
- Firmly attached to the capsule and tibial collateral ligament
Lateral meniscus
- 4/5ths of a circle and uniform width
- Partly blends with the ACL anteriorly
- Anterior and posterior meniscofemoral ligaments (of Humphry and Wrisberg) pass in front of and behind the PCL
- Connected to the medial meniscus anteriorly by the transverse ligament
Variant – Discoid Meniscus
- Almost exclusively lateral meniscus
- Congenital variation of meniscus shape
- Central hypertrophy, larger diameter, discoid shape
- Incidence of 3-5% and more prevalent in Asian populations
- Presentation
- Usually asymptomatic unless unstable or torn
- Examination
- Can have a characteristic ‘clunk’ at 110 degrees when bent and 10 degrees when straightened
- Imaging
- Plain X rays
- Femoral condyle with block shape ‘squaring’
- Increased concavity of tibial plateau
- Widened joint space (> 11mm)
- Hypoplasia of lateral tibial spine
- MRI
- Presence of AP band measuring >5mm in thickness across 3 sagittal sections
- Bowtie shape in sagittal view
- Differences in size between anterior and posterior horn
- Coronal sections showing complete meniscus in AP
- Increase in transverse diameter (>15mm)
- Plain X rays
- Treatment
- Nonoperative
- If asymptomatic
- Conservative approach favoured
- Operative
- Excision
- Arthroscopic partial meniscectomy with saucerization
- Risk of creating unstable joint and secondary osteoarthritis
- Nonoperative

https://en.wikipedia.org/wiki/Discoid_meniscus
Synovial Membrane
- Most extensive in the body
- Anteriorly separated from the patellar ligament by the infrapatellar fat pad
- Herniates into the joint as 2 alar folds
- Converges into a single midline fold – the infrapatellar fold
Bursa
- 4 anteriorly
- 2 on either side
- 4 posteriorly
Blood Supply
- Capsule and joint structures are supplied from the anastomoses around the knee
- Mainly 5 genicular branches of the popliteal artery
- Cruciate ligaments supplied by the middle genicular artery
Nerve Supply
- Femoral nerve
- Sciatic nerve
- Genicular branches of the tibial and common peroneal nerve
- Tibial nerve supplies cruciate ligaments sensation
- Obturator nerve
- Twig from posterior division
- Accompanies the femoral artery through gap in adductor magnus
- Twig from posterior division
Movements
Flexion
- Performed by the hamstrings
- Assisted by gracilis, sartorius, popliteus, gastrocnemius and plantaris
- Limited to about 150 degrees by soft tissue
Extension
- Performed by quadriceps
- Assisted by tensor fasciae latae
- Lateral femoral condyle completes extension excursion 30 degrees short of full extension
- Then it rotates forward around a taut ACL, while medial condyle glides backwards
- This is part of a passive ‘locking’ mechanism which secures the joint in 5-10 degrees of hyperextension
- To ‘unlock’ the joint, popliteus medially rotates the tibia
Medial rotation of the tibia
- By semimembranosus and semitendinosus
Lateral rotation of the tibia
- Produced by biceps femoris
References
Last, R. and McMinn, R., 1994. Last’s Anatomy. 9th ed. Edinburgh: Churchill
Solomon, L., Warwick D. and Nayagam S. 2001. Apley’s System of Orthopaedics and Fractures. 8th ed. Great Britain. Arnold
Reider B. 1999. The Orthopaedic Physical Examination. Pennsylvania. W.B. Sauders Company
Saavedra, M., Sepúlveda, M., Jesús Tuca, M., & Birrer, E. (2020). Discoid meniscus: current concepts. EFORT Open Reviews, 5(7), 371-379. doi: 10.1302/2058-5241.5.190023
Markatos, K., Kaseta, M., Lallos, S., Korres, D., & Efstathopoulos, N. (2012). The anatomy of the ACL and its importance in ACL reconstruction. European Journal Of Orthopaedic Surgery & Traumatology, 23(7), 747-752. doi: 10.1007/s00590-012-1079-8
Author Contributions
Matthew Sun, medical student, Western Health 2021