Introduction
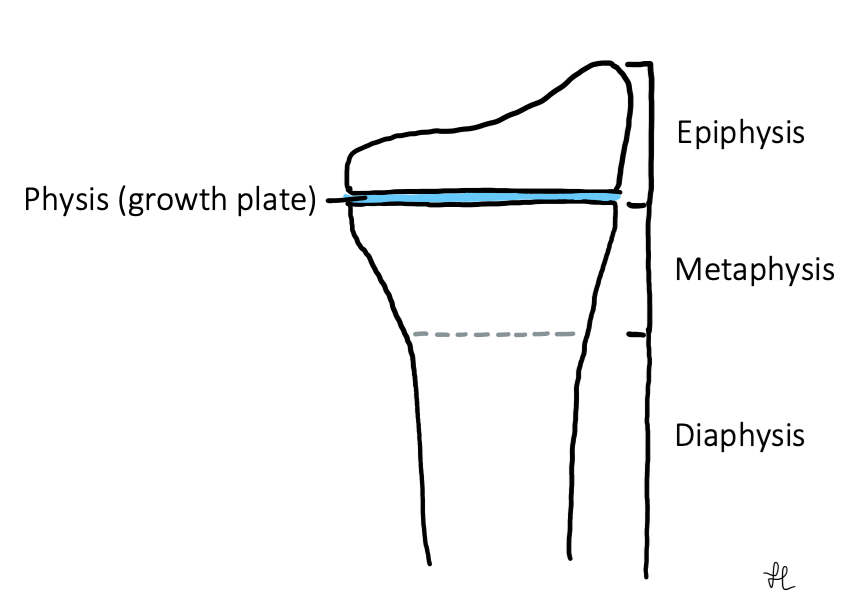
The Salter-Harris classification system is used to grade fractures that occur in children which involve the growth plate (‘physis’) of a long bone (e.g. tibia or humerus). The classification is based on the involvement of the metaphysis, physis or epiphysis.
Salter-Harris fractures are usually the result of a traumatic incident, like a fall. An underlying bone infection (e.g. osteomyelitis) may also present as a Type V injury. Physeal injuries have the potential for growth disturbance, growth arrest and resulting deformity. In some cases, intervention may be required to prevent premature physeal closure.
Classification System
There are 5 most common types of Salter-Harris fractures (Types I to V). They increase in severity, with the higher type number being associated with more interventions, complications and worse prognosis.
The mnemonic S-A-L-T-ER is commonly used to recall the fracture patterns.
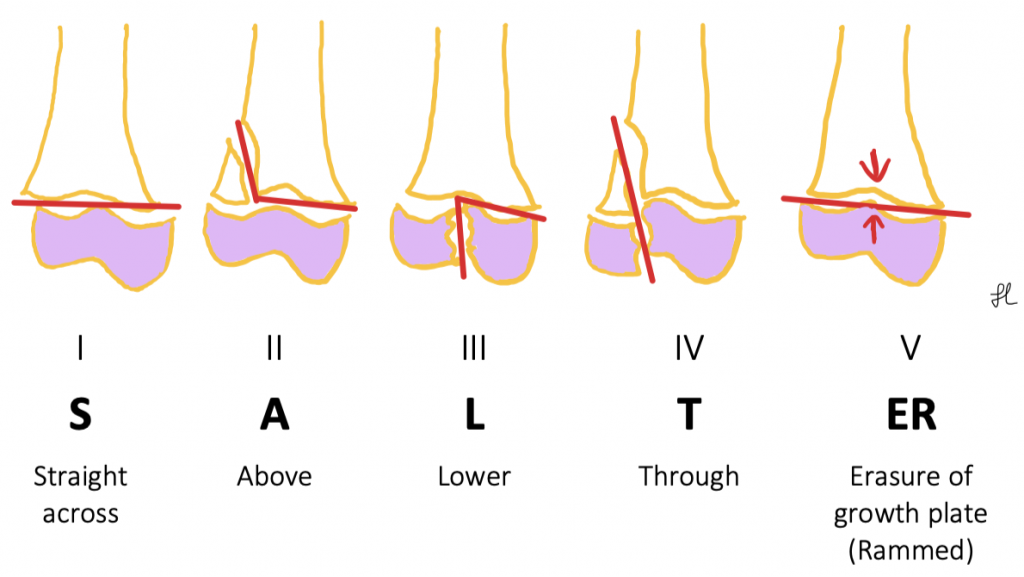
| Type I | – Through the growth plate – More common in younger patients with thicker physis – Fast healing, rare to have complications |
| Type II | – *Most common type – Through growth plate and metaphysis, spares the epiphysis – Creates a separate metaphyseal fragment, called the ‘Thurston-Holland’ fragment – Fast healing |
| Type III | – Through growth plate and epiphysis, spares the metaphysis – Creates an intra-articular fracture – Requires anatomic reduction and internal fixation |
| Type IV | – Through growth plate, epiphysis and metaphysis – Possible growth disturbance and angular deformity – Requires anatomic reduction and internal fixation |
| Type V | – Rare – Compressive injury to the growth plate (e.g. crush injuries) – No associated fractures of the epiphysis or metaphysis – Possible permanent growth arrest |
Examination
- Pain and swelling around the end of the long bone
- Limited ROM
- Limited ability to weight bear
- Possible bone deformity
- *Assess neurovascular status, especially distal to injury (pulse, sensation, power)
Investigation
- Imaging
- X-rays are the primary imaging modality of choice
- A CT scan may be useful in appreciating fracture displacement and configuration (e.g. fracture in >1 plane)
- An MRI may be useful for detecting subtle changes if X-rays are normal but there is a high index of clinical suspicion for an injury
- Type I fractures can be harder to visualise on X-ray. It occasionally identifies as a minor separation of the epiphysis from the bone. Diagnosis is based on clinical history and exam findings. Might be picked up on X-ray a few weeks post-injury
- Type V fractures are often missed as it involves only injury to the growth plate and no physical fractures. Typically diagnosed retrospectively when patient presents for follow-up visits with evidence of growth disturbance/arrest
- X-rays are the primary imaging modality of choice
Management
- Initial treatment: Rest, ice, elevate to reduce swelling
- Analgesia (start with NSAIDs)
- Type I & II: typically managed by closed reduction to set the bone into position without the need for surgery, followed by plaster immobilisation (e.g. slab/cast)
- Type III & IV: typically managed by open reduction and internal fixation
- Type V: focus is placed on managing the subsequent growth disturbance/arrest
- Review in clinic at 1 week, unless otherwise instructed by Ortho
References
Aziz F, & Doty C.I. (2017). Orthopedic emergencies. Stone C, & Humphries R.L.(Eds.), CURRENT Diagnosis & Treatment: Emergency Medicine, 8e. McGraw Hill. https://accessmedicine.mhmedical.com/content.aspx?bookid=2172§ionid=165061678
Cepela, D. J., Tartaglione, J. P., Dooley, T. P., & Patel, P. N. (2016). Classifications In Brief: Salter-Harris Classification of Pediatric Physeal Fractures. Clinical orthopaedics and related research, 474(11), 2531–2537. https://doi.org/10.1007/s11999-016-4891-3
Levine, R. H., Foris, L. A., Nezwek, T. A., & Waseem, M. (2021). Salter Harris Fractures. In StatPearls. StatPearls Publishing.
Author Contributions
Julia Liew, Medical Student, Western Health 2021