Journal Club
March 2010
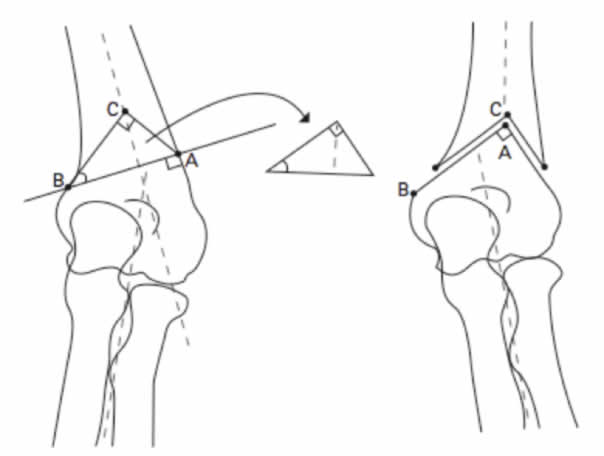
Reverse V osteotomy of the distal humerus the correction of cubitus varus
Yun YH, Shin SJ, Moon JG.Department of Orthopaedic Surgery, Ewha Womans University, Mok-dong Hospital, 911-1, Mok-dong, Yangcheon-gu, Seoul 158-710, Korea.
J Bone Joint Surg Br. 2007 Apr;89(4):527-31
Reviewed by
Dr Josh Petterwood
MBBS | Accredited Orthopaedic Registrar
Introduction
- Case series/technical note
Methodology
- Pre-operative planning
- Full length XR both arms
- Humeral-elbow-wrist angle both arms
- Valgus +, varus –
- Amount of correction required based on contralateral arm
- Osteotomy planned
- Correction of lateral/medial prominence
- Full length XR both arms
- Procedure
- Tourniquet, lateral, elbow 90° flexion
- Posterolateral approach
- Goniometer
- ABC resected
- Lateral rotation of distal segment
- Lateral crossed K-wire and wiring
- 90° slab for 2/52 then active ROM
- Evaluation
- Radiologically
- Correction of deformity based on humeral-elbow-wrist angle
- Lateral prominence (X-Y)
- Clinically
- ROM
- Complications
- Rated as excellent/good/poor according to Oppenheim
- Radiologically
Results
- 22 children with cubitus varus
- 19 boys, 3 girls
- Mean age 9.5
- 17 supracondylar, 2 lateral condylar, 2 medial condylar, 1 physeal seperation
- All children had good elbow function and full ROM
- Indication was cosmetic deformity
- 20 excellent, 2 good (at mean follow up 16/12)
- All osteotomies united at 10 weeks
- Mean pre-operative deformity
- -16.9 (-25 to +9)
- Post-operatively
- +7.3 (-2 to +14)
- Mean correction 24.1 degrees
- 2 with lateral prominence (mild < 5mm)
- 1 intra-operative fracture
- 1 ulna nerve palsy
Discussion
- Many approaches/osteotomies/fixation described
- Perceived advantages of reverse V
- High. Providing better fixation. Particularly in adult.
- Inherently stable
- Easy and precise assessment/correction of lateral prominence through pre-op plan
- Fixation
- Lateral crossed K-wires with supplemental wiring
- Reduced chance of iatrogenic nerve injury
- Stable enabling active ROM to begin at 2 weeks
Pros of Study
- Well described Case series/technical note
Take home message
Reverse V osteotomy is a potential technique for correction of cubitus varus deformity in children
Webpage Last Modified:
30 June, 2010
