Journal Club
June 2010
Concomitant Arthroscopic SLAP and Rotator Cuff Repair
Brian Forsythe, MD, Daniel Guss, MD, Shawn G. Anthony, BS, and Scott D. Martin, MD
Harvard Medical School and Brigham and Women’s Hospital, Boston, Massachusetts
J Bone Joint Surg Am. 2010 Jun;92(6):1362-9.
Reviewed by
Dr Eugene T.H. Ek
PhD, MBBS | Senior Accredited Orthopaedic Registrar
Introduction
- Concurrent SLAP repair and RC repair is controversial especially in middle aged patients
- Options
- Biceps anchor tenotomy
- Biceps tenodesis
- Biceps tendon repair
- Aim
- To determine whether concomitant arthroscopic repairs of a rotator cuff tear and a SLAP lesion can yield satisfactory outcomes comparable with those seen with rotator cuff repair alone.
Methodology
- Retrospective review - 2003-2005
- Consecutive series
- 34 patients - combined RCR and SLAP repairs
- 28 patients – RCR alone
- Exclusion criteria:
- Mini-open or open procedure
- History of ipsilateral shoulder surgery
- Grade III/IV glenohumeral OA
- Massive rotator cuff tear/pseudoparalysis
- Adhesive capsulitis
- Advanced fatty infiltration or atrophy
- Surgery by single surgeon
- Independent review
- RC tear and SLAP lesion
- Confirmed with MR arthrogram and positive O’Brien’s test
- RC tear without SLAP lesion
- Confirmed with MR arthrogram and negative O’Brien’s test
- SLAP lesions repairs
- 32 type II
- 1 type IV
- 1 type V (SLAP with Bankhart)
- Rotator cuff repair only
- 3 had arthroscopic biceps tenodesis for tear >30% diameter
- 5 patients had type I SLAP - debrided
- Technique:
- All arthroscopic double row rotator cuff repairs
- SLAP repaired with arthroscopic suture anchors
- Post op:
- Day case
- Abduction pillow 15degrees
- Pendular movement 2 weeks
- Passive movements till 6 weeks
- Active movements after 6 weeks
Results
- Rotator cuff cohort
- 15 men, 13 women
- average age of 59.6 ± 7.9 years (range, 43-75)
- Rotator cuff and SLAP cohort
- 21 men, 13 women
- average age of 56.9 ± 7.9 years (range, 43-75)
- Return to work
- 22/25 (rotator cuff only cohort)
- 29/30 (rotator cuff & SLAP cohort)
- Return to sport
- 16/18 (rotator cuff only cohort)
- 29/31 (rotator cuff & SLAP cohort)
Discussion
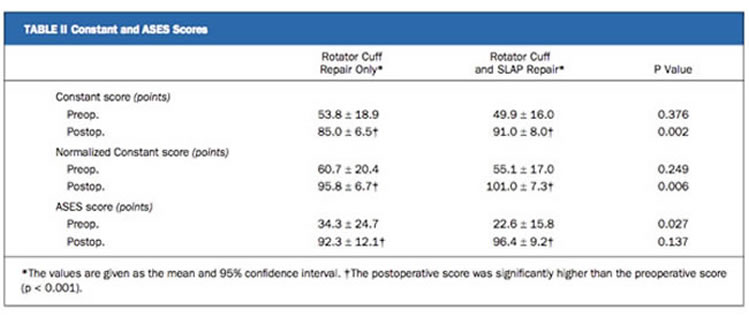
- Patients with combined SLAP and RC tears had lower functional scores preoperatively compared to patients with RC tear only
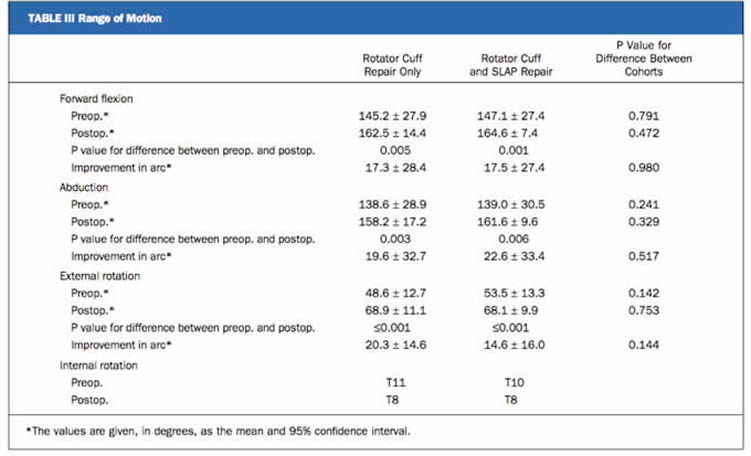
- Postoperatively, patients with combined repairs had:
- similar or better functional results compared to rotator cuff repair alone
- Similar range of motion
Pros of Study
- Only study to compare RC repair and SLAP with RC repair only
- Single surgeon
- similar technique
- Standardized postop regime
Cons of Study
- Retrospective review
- Small numbers, No power analysis
- Average age of patients ~60 years old (generally older that normal for SLAP repair)
- No early or intermediate follow up
- Single surgeon – decreases generalizability of results Imaging was not performed to confirm healing of the repairs
- No comparison between RC repair without SLAP repair compared to combined RC repair and SLAP repair
Journal club Discussion
- The function and role of the biceps tendon and it’s anchor is largely unknown
- There is a perception that SLAP repairs do cause stiffness post op and is associated with difficult rehabilitation
- Generally SLAP repairs should be done in younger patients who are active and highly motivated to undergo the intense rehabilitation
- The Patients in this study are generally older (ave age 60yo) that the normal age in which SLAP repairs are usually done
Take home message
- Combined SLAP and RC repairs may provide similar results compared to RC repairs alone
- SLAP repairs with RC repairs may not increase shoulder stiffness or reduce shoulder function
Webpage Last Modified:
30 June, 2010
